

Cancer Treatment And A New Smile
The Double-Edged Sword of Cancer Treatment
Meet Will, whose successful treatment for throat cancer eight years ago gave him a new lease on life. Unfortunately, it exacerbated a dental problem that started before his treatment: worn and eroded teeth.
 |
| Will’s teeth are chipping and unaesthetic as a result of wear, dry mouth and acidity. |
“My teeth looked terrible. I was having constant sensitivity and was having a hard time eating,” he said.
It is actually quite common for cancer patients to experience oral side effects — especially those receiving radiation therapy to the head and neck, as Will did. Cancer treatments such as chemotherapy and radiation work by attacking cancer cells. However, normal cells can be affected as innocent bystanders. In Will’s case, the radiation treatments aimed at his head and neck also affected his salivary glands, creating a condition known as xerostomia (“xero” – dry; “stomia” – mouth).
Among its many functions, saliva protects teeth from acids in the mouth that constantly bathe the teeth. Without that protection, the acids from foods and beverages — and certain strains of decay-causing bacteria that feed on sugar — will start to dissolve the hard enamel covering of the teeth. Once the enamel is gone, it will not come back. Will was unknowingly compounding his problem by frequently sipping acidic beverages: sodas or tea with lemon to moisten his mouth to overcome the constant dryness.
 |
| Wear and erosion leads to loss of the outer enamel cap that protects the teeth, and results in exposure of the softer inner dentin. |
 |
| As the back teeth wear excessively, the bite deepens resulting in over-closure of the jaws, and discomfort. |
As if the absence of protective saliva and the constant contact with acidic drinks were not stressing him and his teeth enough, Will had developed gastro-esophogeal reflux disease (GERD), also from the cancer treatment. GERD causes acid regurgitation from the stomach into the mouth, where it erodes the teeth. It’s not surprising, then, that all of Will’s teeth (except the few that happened to be covered with dental crowns) showed significant erosion. Because missing enamel provides an entry point for decay-causing bacteria, many teeth were also starting to decay.
When a significant amount of enamel is thus destroyed, the softer inner tooth material known as dentin becomes exposed, which erodes even more quickly. As a consequence of a substantial loss of tooth structure, the teeth may appear misshapen, too small, and/or discolored. Will’s erosion had produced overclosure of his bite, meaning that because his teeth were so worn, his jaws had to close more than normal in order to get the teeth to bite together. Eroded teeth can also become sensitive to hot, cold and touch. This uncomfortable sensitivity, along with the unaesthetic appearance of his teeth, prompted Will to seek consultation for a smile makeover.
“I want to be able to smile again,” he said.
Mapping a Route to Successful Treatment
My first step was a thorough assessment of Will’s situation. The conditions in each person’s mouth are different, even if the overriding complaint — erosion, for example — is the same. I knew that covering his severely eroded teeth with beautiful dental crowns might be a good option, but before recommending this I needed to know what the conditions were in his mouth that might jeopardize a good result, and decide what was best for Will. So I carefully examined his mouth for red flags in four fundamental categories: periodontal risk, biomechanical risk, functional risk and aesthetic risk.
Periodontal Risk — refers to the supporting structure of the teeth, i.e., the gum tissues and bone. Will’s gums were relatively healthy and his tooth-supporting bone had not deteriorated along with his teeth, so his risk in this category was low.
Biomechanical Risk — relates to integrity of tooth structure, the teeth themselves. This was the biggest red flag in Will’s case because of the severe enamel erosion, caries (tooth decay), and lack of saliva. His tooth decay would surely progress if we did not act fast. As a preliminary step, I removed the decay from his teeth and then filled them with a glass ionomer filling material. This is one of the newer temporary filling materials; it has the added advantage of releasing fluoride, which strengthens the teeth against further decay.
Importantly, Will was prescribed a caries (tooth decay) prevention protocol, necessary to change the conditions that lead to decay, which included:
- Using a mouthrinse to counteract acidity and to make his mouth more basic (the opposite of acidic), thereby discouraging the growth of acid-producing bacteria
- Rinsing with fluoride solutions and applying fluoride varnishes to strengthen tooth structure and make it more resistant to acid dissolution and decay
- Using salivary replacement/stimulation medication to counteract dry mouth
These measures would make him more comfortable right away and reduce his risk of further tooth structure loss by decay and or/erosion.
Functional Risk — describes how teeth, muscles and jaw joints are working. Loss of tooth structure throughout his mouth because of erosion and decay had caused Will’s bite to over close; but this could be addressed by rebuilding his teeth. Will’s dental function otherwise was acceptable with normal opening and range of motion, and no symptoms of jaw-joint or muscle pain.
 |
| Will has a “high smile line,” which means he shows a lot of his teeth and gums when he smiles, putting him in a high aesthetic risk category. |
 |
Aesthetic Risk — having a high risk in this category simply means that relatively speaking, either too much or too little of the teeth or gum tissue is on display in the smile. One of Will’s main complaints was that his teeth appeared shortened, worn, chipped, and stained. In people whose lips don’t move much when they talk or smile, purely cosmetic issues of the teeth and gums are not as problematic. But Will’s “high smile line” meant that any aesthetic problems with his teeth would be obvious. This would surely influence the plan of action.
A New Smile
After a thorough evaluation of Will’s individual risk factors, I determined that the best treatment would be to rebuild all of his teeth with dental crowns, made out of lifelike porcelain for the most natural, long-lasting and aesthetic results. This would restore his bite while also protecting his teeth as best as possible from further erosion — and give him a great-looking smile. He would of course need to continue using his caries-prevention and salivary replacement/stimulation products while minimizing use of acidic beverages — for the rest of his life.
Because Will’s teeth were so worn down, his jaw muscles had developed new ways of working to compensate for the deficiency. I fitted him with a special bite appliance that would re-train his muscles to work more naturally. Helping the jaw muscles relax would also allow me to determine the most comfortable and functional size and shape for his new crowns. Once I had this information, along with models (exact-size replicas) of Will’s teeth, I sent it to a dental laboratory so the dental technicians with whom I worked on his case could create a mock-up of what Will’s fully restored teeth would look like.
 |
| A close-up view of Will’s front teeth before treatment. |
 |
| Will with his new “trial smile.” These temporary crowns can be tried for eating, comfort, speech and aesthetics and modified if necessary, before committing to final crowns. |
When the mocked-up teeth came back from the lab, we recreated them in Will’s mouth to give him what’s known as a “trial smile.” By fabricating temporary acrylic crowns that duplicated the laboratory models, we showed him what his restored teeth could actually look and feel like. A trial smile is the best way to make sure the final results will work and that all expectations will be met. Will and I were able to evaluate the fit of each crown before the treatment was made permanent and irreversible. After I made some minute but important adjustments, I sent records of the adjustments back to the lab, where they were incorporated into the creation of the final crowns.
I then needed to prepare Will’s teeth to receive the crowns. This involved some shaping with a dental drill to ensure proper fit. Afterwards, I cemented each crown in place, a process that took two appointments and a total of six hours. When I handed Will the mirror, he was speechless!
A Better Quality of Life
Will loves his new smile and his quality of life has improved remarkably.
 |
 |
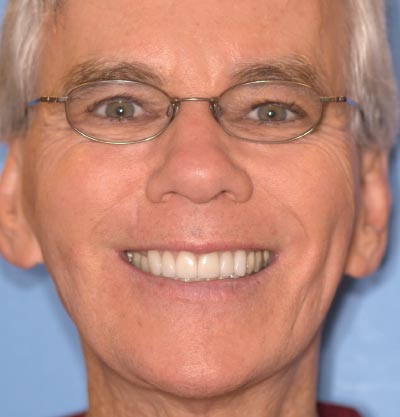
| A beautiful smile was created that fits Will’s facial shape, creating a very natural look. The teeth have been restored to perfect size, shape and color. |
“I am so excited to have a great smile again,” he said. “It is amazing to be able to smile and eat confidently. Thank you, Dr. Bynum for restoring my confidence!”
Will knows that as a cancer survivor, his dental problems are not over. His xerostomia and exposure to acids can’t be completely eliminated, so he is still at high risk for decay, particularly at the gum line where the crowns meet the natural tooth structure. Without the natural protection of saliva, he will have to be meticulous about his oral hygiene, the use of the prescribed fluoride and other rinses, as well as adhering to a schedule of regular dental checkups so his oral and dental health can be monitored. Still, the treatment we chose has helped to manage his condition, giving him an opportunity to keep his smile attractive and his teeth healthy throughout his life.
